Understanding your unique eating behaviour phenotype helps you to identify why you eat, what drives your weight gain and prevents you from achieving lasting weight loss success.
Your eating drivers or motivation to eat are those inert signals that compel you to eat and that may overwhelm your willpower during any dieting attempt.
Please ask yourself
Why do I eat? What motivates me to eat?
What are the internal drivers that propel me to eat in different situations?
Please add one sentence.
What are eating behaviour phenotypes?
Eating behaviour phenotypes are observable patterns or traits of how people behave in relation to food.
A person's genetic predispositions determine some of these phenotypes related to weight gain.
Others are learned behaviours and are related to environmental factors.
Eating behaviour phenotypes can be divided into three main groups.
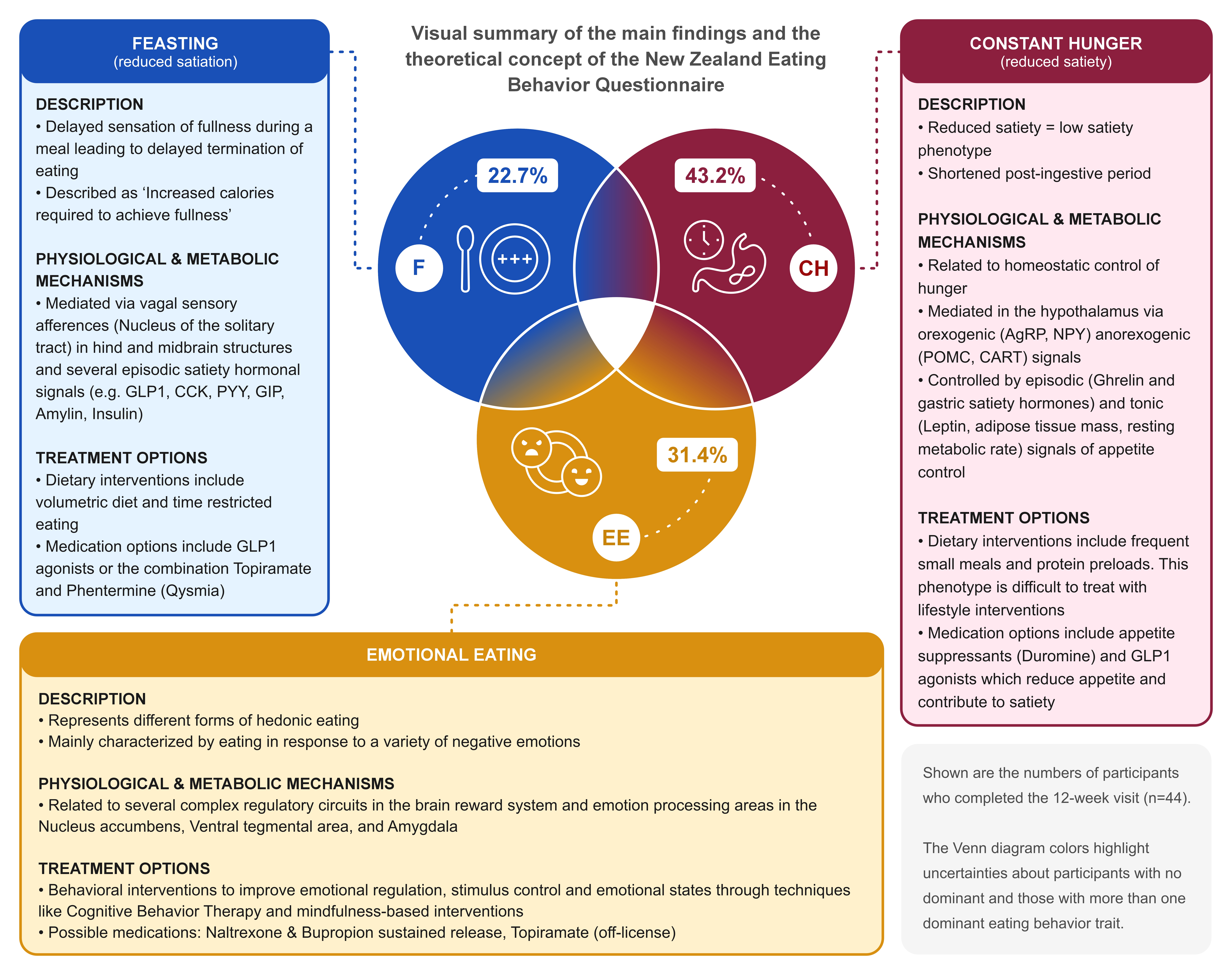
1. Feasters or reduced satiation
The absence of the feeling of fullness during meals can lead to larger portion sizes and overeating.
Ask yourself – do you get a good sense of fullness during a meal?
Satiation is the feeling of fullness that tells your brain to stop eating. Reduced satiation makes it challenging to recognise when to stop eating, leading to delayed meal termination and unwanted overeating.
Satiation is determined by satiety hormones derived from your gut that relay to your brain a sense of fullness, and that slow the emptying of your stomach.
Adaptations of those satiety hormones are used in modern weight-management medications that work best in individuals with this dominant phenotype.
The questionnaire will determine the extent of your degree of feasting-type eating behaviour.
Constant Hunger or reduced satiety
Struggling with a powerful hunger sensation between meals
Ask yourself: Do you get hungry when you haven’t had a meal in a while?
Satiety is the sensation of fullness and not wanting or needing to eat.
Having a reduced satiety phenotype means that you frequently struggle with hunger and often look for food.
You may also notice an early return to hunger after a meal.
Satiety is related to the transit of food through your stomach, the background level of hunger hormones, and your metabolism.
Certain weight management medications and dietary modifications can help with this sensation and allow greater control over your eating.
The questionnaire will assess your degree of constant hunger-type eating behaviour.
Emotional Eating
A strong desire for comfort foods to deal with emotional triggers
Ask yourself – do you use food to make you feel better, to comfort you or to reduce stress?
Emotional eating occurs when you use food to cope with your emotions rather than to address hunger; you eat to make yourself feel better.
Food can be a coping mechanism when you feel sad, bored, lonely or unduly stressed.
Such a behaviour can be measured with questionnaires and may be related to past and present experiences, and emotional states such as low mood and anxiety.
Interventions such as cognitive behavioural therapy and certain medications that address these eating behaviours or related psychological problems may help.
Identifying whether you exhibit some of these eating behaviours through the questionnaire may support your weight loss success.
How the questionnaire works
The questionnaire is straightforward. Try the training and instruction pages to understand the test.
We will ask you specific questions related to your eating behaviours or habits.
Questions are presented on continuous scales or sliders, and we ask you to place the cursor on the point that best represents your general perception or feeling.
There are also image questions that will be explained as you go along.
You must allow yourself sufficient time to reflect on the question before you answer.
What will happen once you have completed the questionnaire?
How do we calculate your unique eating behaviour scores?
We will use your answers to calculate your eating behaviour type and compare the strengths of your eating behaviours with a reference population, telling you whether you have more powerful drivers to eat than others.
We know that this relates to your body weight and your likelihood of succeeding with weight loss.
Results will be presented in easy-to-understand graphs at the end of the test.
We also use AI to translate your results into personalized recommendations based on your unique eating behaviors (future feature).
We will provide general recommendations; however, the decision to discuss and implement any suggestions will be left to you and your healthcare professional.
How to use the results for your weight loss journey?
Identify your unique eating behaviour phenotype to improve your long-term weight loss
Your unique eating behaviour phenotype can be assessed with the questionnaire
It can guide your health care professional to find the most suitable diet and weight management medication for you
You can track how your eating behaviour changes in response to medications, finding out early whether the medication you use is having an effect and will lead to weight loss
Increases your awareness of eating behaviours in your day-to-day routines, as this can lead to behaviour change and sustainable success
Clinical studies
Articles in peer-reviewed journals of the New Zealand Eating Behaviour questionnaire for phenotype-guided treatment allocation.
The New Zealand Eating Behaviour Questionnaire was validated in three large cohorts of patients with obesity related complications.
The questionnaire had good internal reliability, validity and reproducibility.
The latest study of the research team revealed twice as much weight loss in patients treated with medication matching their dominant eating behaviour phenotype identified in the NZ-EBQ, compared with an eating behaviour incongruent medication use.
The medication studied is called Contrave™ (Naltrexone/Bupropion combination) and had greater benefit for patients with an emotional eating phenotype compared with those with a reduced satiety phenotype.
The knowledge gained through phenotyping supports clinicians in using the most appropriate medication for their patients, which is a step towards a precision medicine approach.
The study titled “Applicability of the New Zealand-Eating Behaviour Questionnaire to predict
weight loss responses to naltrexone/bupropion: a proof-of-concept trial” published in December
2025 in Obesity Pillars, the journal of the American Obesity Medical Association, examined
whether specific eating behaviour types can predict weight loss response to the naltrexone/
bupropion combination (Contrave™), a pharmacotherapy designed to modulate the brain’s
reward system and hypothalamic hunger pathways.
The researchers stratified participants into three distinct eating phenotypes based on NZ-EBQ
scores: (1) emotional eaters, (2) those with reduced satiety (chronic hunger and feeling hungry
again soon after meals), and (3) those with reduced satiation (difficulty stopping eating).
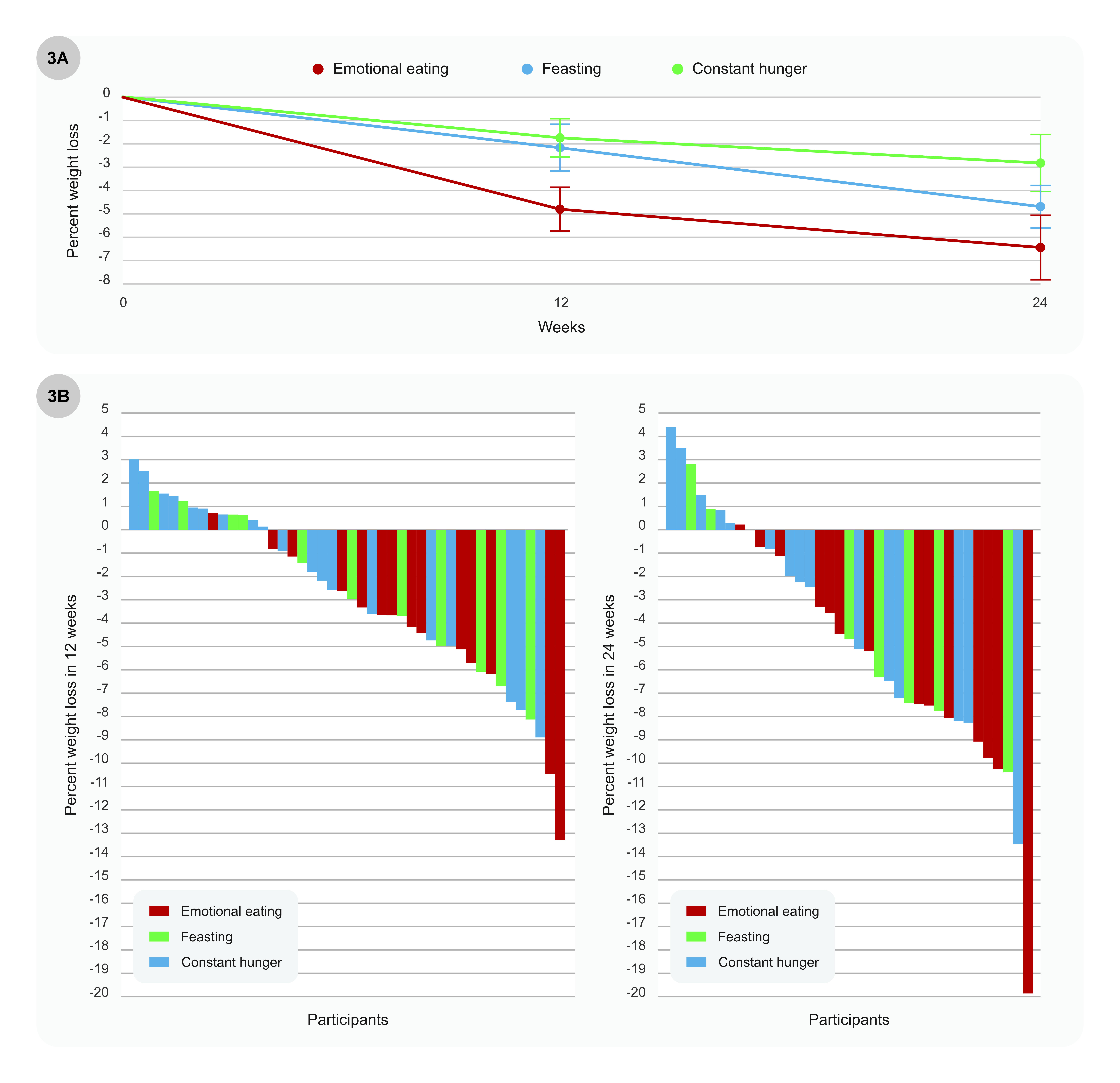
In this 24-week clinical study, the average weight loss across participants was approximately
4.5% of initial body weight, consistent with the expectations for this medication. However,
emotional eaters achieved a significantly greater weight loss of 6.44% compared to those with
other eating behaviours (reduced satiety), who experienced only a modest average weight loss of
2.8%, and several of them experienced a weight increase while on the medication.
These results show that the NZ-EBQ effectively identifies patients whose weight gain is primarily
driven by emotions and food cravings, the specific pathway targeted by Contrave™, suggesting
that the medication may work particularly well for people with this eating behaviour.
The results support the concept of precision obesity treatment, where assessment of eating
behaviour can inform medication selection. Larger studies are needed, but the NZ-EBQ shows
promise as a practical tool to personalise obesity management in clinical practice.
Figure 3 from the publication.
Participants with emotional eating achieve greater weight loss with Naltrexone/Bupropion
combination compared with participants with constant hunger and feasters.
Panel A shows the average weight loss from baseline among participants at 12 and 24 weeks
Panel B shows a waterfall plot of the weight loss of individual participants whereby each bar
represents one participant.
The New Zealand eating behavior questionnaire - Validation
study for a novel assessment tool to describe actionable
eating behavior traits.
Here, researchers tested whether the New Zealand Eating Behaviour Questionnaire (NZ-EBQ) could
identify individual eating behaviour patterns. The NZ-EBQ looks at three main eating behaviours:
Feasting – finding it hard to stop eating once you start
Constant hunger – feeling hungry again soon after eating
Emotional eating – eating more when feeling stressed, sad, or upset
This study included people living with obesity, some of whom were on weight-loss medications. The
researchers checked whether the questionnaire could reliably measure the three eating behaviours.
Participants' answers were mostly consistent when they repeated the survey later, especially for
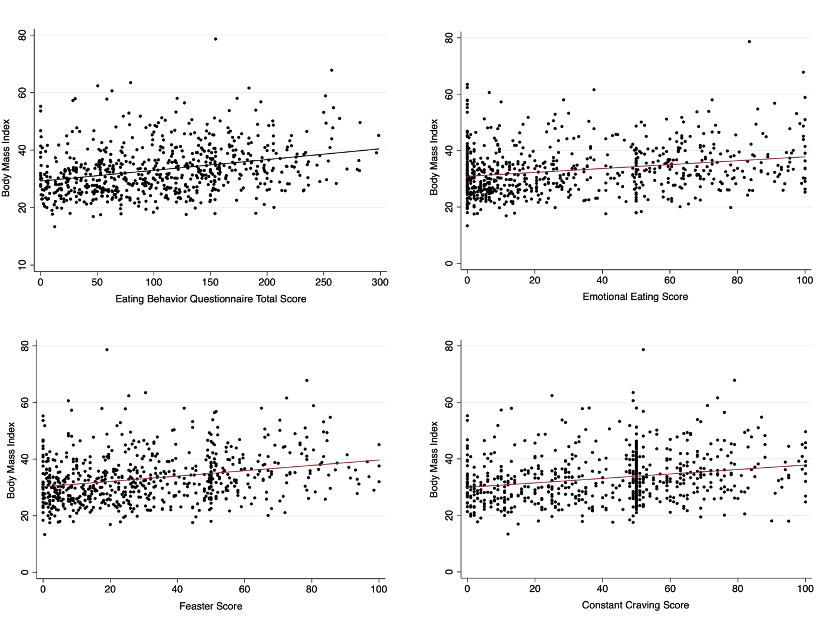
emotional eating. When examining body weight, the study found that higher scores on any of the three
eating patterns were associated with higher body mass index (BMI).
Figure 3 from the publication.
The relationship between participants EBQ total score (the sum of the three EB scores),
and eating behavior specific scores on the NZ-EBQ (0–100) compared to Body Mass Index
(kg/m2)
Overall, the findings show that the NZ-EBQ is a reliable tool for identifying personal eating behaviour traits. The results may help healthcare professionals better understand what drives someone's eating, for example, whether
emotional eating or constant hunger plays a bigger role. This can help to tailor treatments such as lifestyle advice, nutrition support, or medication more precisely to each person's needs.
Schmiedel O, Ivey M, Murphy R. Broader Validation of New
Zealand Eating Behavior Questionnaire as Clinical Assessment
Tool to Identify Actionable Eating Behavior Traits.
Nutrients. 2025 Mar
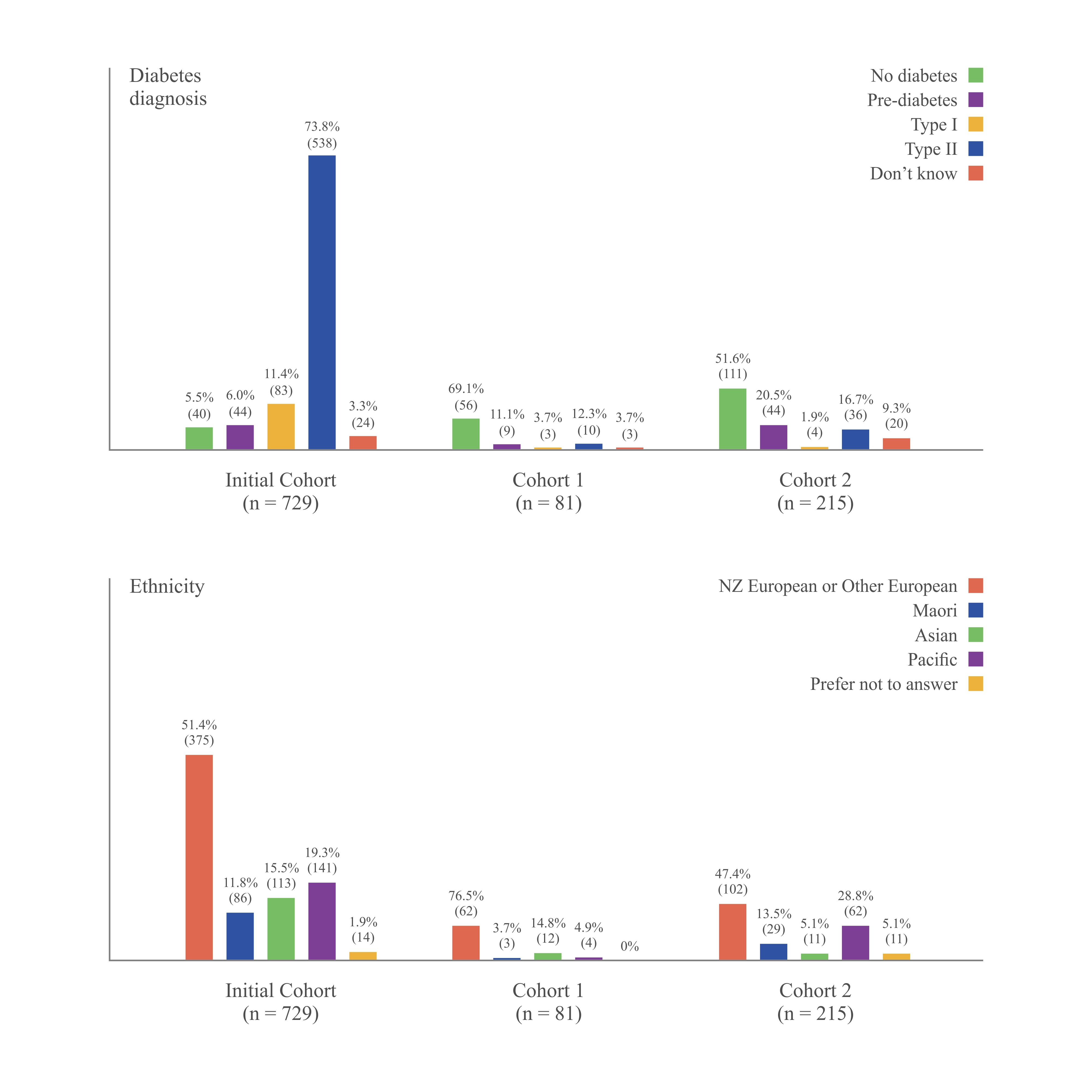
This study took the New Zealand Eating Behavior Questionnaire (NZEBQ) to the next level,
testing it in two separate more diverse groups, including people with higher body weight and
different ethnic backgrounds.
Unlike the earlier study, it focused on real-world reliability and how well the questionnaire
captures three key eating patterns: feasting, constant hunger, and emotional eating.
The results showed it works consistently across different people, with higher scores linked to
higher body weight.
This means the NZEBQ can help clinicians identify individual eating traits and design more
personalized strategies for managing weight.
Figure 3 from the publication.
Prevalence of Diabetes and Ethnicity of Participants in the Two Cohorts of this study compared to
Initial Cohort (first paper). The values are depicted as a percentage of participants within each cohort.
The absolute number of participants is provided for reference.
How testing works
The four steps of the test
Step 1
Practice how to take the test
Slider questions
Place the cursor on the point that best represents your general perception or feeling about the question.
Definitely FALSEUndecidedDefinitely TRUE
Image questions
There will be different image-based questions. Please follow the instructions and answer the questions.
You will be shown an image and asked about your preferences, thoughts and feelings.
Please take as long as you need, answer as honestly as possible, reflecting on how you think about the image and how it makes you feel.
Step 2
Take the Pretest – My hunger and fullness sensation RIGHT NOW
Step 3
The main questionnaire - instructions
Are you ready to take the test?
Be as honest and accurate with your answers as you can.
There are no right or wrong answers.
Step 4
End of questionnaire
Demographics
Please tell us a bit about yourself to help interpret your Eating Behaviour score.
Thank You!
Thank you for taking the time to complete the questionnaire. Your responses will help us calculate your unique eating behaviour phenotype.
Here we are asking for height and weight data to calculate your Body Mass Index (BMI) to interpret your individual data in a broader context.
This response helps you understand how your unique eating behaviour relates to your BMI and to the background population.
Your responses will remain completely anonymous. No personally identifying information will be collected, and your answers cannot be traced back to you. We will only collect aggregated data and trends, and your individual answers will remain confidential.
Your Honest Input Matters
Please provide correct answers as we need to use the data to calculate your results.
Many thanks for providing the information.
Disclaimer
Your personal Eating Behaviour Score – General Information
Use your score to start or redirect your weight loss journey. The NZ-EBQ calculator is
currently open access and free to use by anyone interested in their unique eating
behaviour, whether they are on obesity medications or not (link to the legal aspect).
The NZ-EBQ does not give or replace medical advice or medical information. Your eating
behaviour score is not a diagnosis of a particular medical condition or of the underlying
causes of your weight, as your weight will be affected by many other factors.
There are no ‘good’ or ‘bad’ results; the questionnaire is designed to describe eating
patterns, not to judge or diagnose. Your responses may help guide future discussions,
support options, or research related to eating behaviour.
You should always talk to your doctor or other healthcare professional about any
health problems you may be suffering from.
What will we do with your data?
We will use the answers you provide to calculate your unique eating behaviour score
and to provide you with a summary of your information on how your score compares
to others.
By using the NZ-EBQ calculator, you consent to us using your information for this
purpose. We do not share that information with any third party other than the service
providers who securely holds the data.
With your consent (optional), we will use your data for non-commercial research
purposes. For example, we may publish research into eating behaviours that uses this
information; however, this is not a research study. We may also use it to improve the
NZ-EBQ.
Further information about your rights in relation to your data and how to contact us
are set out in our privacy policy.
See our Privacy Policy to learn how we protect your data.
Be part of our ongoing research.
We would appreciate it if you could contribute the information you have provided
when using the NZ-EBQ today to future research into eating behaviours and the
usefulness of the NZ-EBQ. Please note this is not a research study.
Your consent is completely optional (you will get the same results either way). You
may withdraw your consent at any time. For more information see our Privacy Policy.
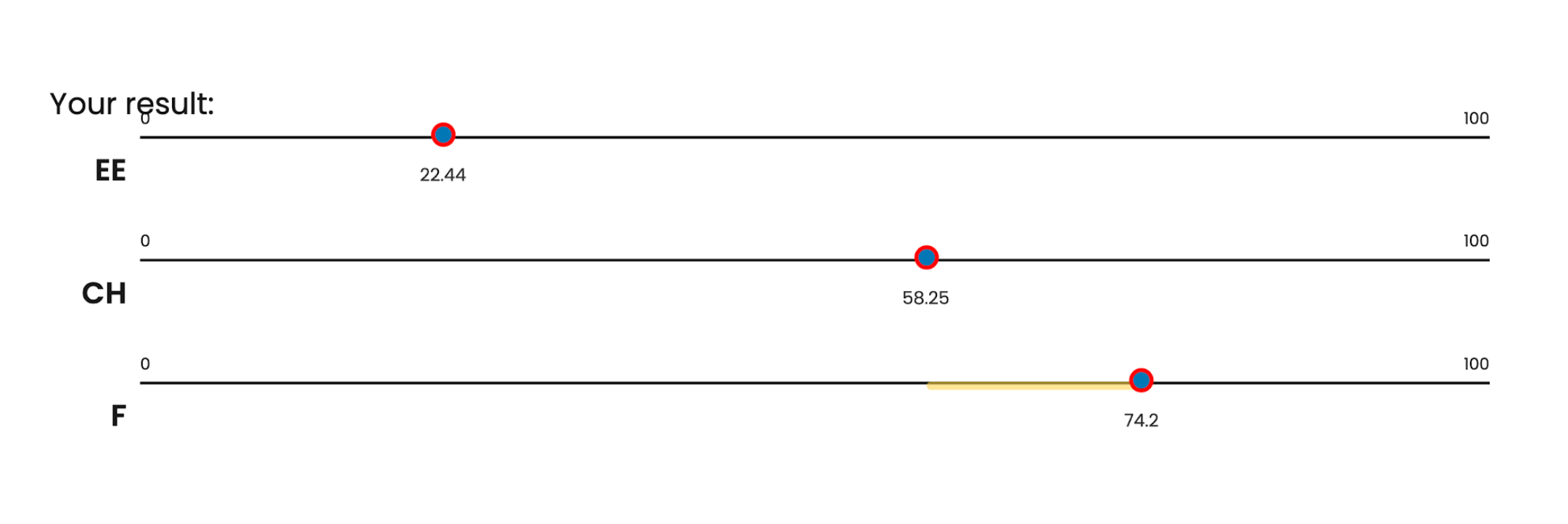
Visual Analogue Scales (0-100)
Your results:
EE
0
100
CH
0
100
F
0
100
How to understand these scales
Each scale shows a different aspect of your eating behaviour.
The three scales have been constructed based on your answers in the questionnaire
Between 7 and 10 questions contribute to one scale (EE, CH and F)
There are no right or wrong scores.
Each scale runs from 0 to 100.
0 means very low on that scale
100 means very high on that scale
The number shows where your results sit along that line
For example:
For a person with the ‘Feasting’ eating behaviour type (difficulty in stopping eating or eating large portions), the results may look like:
Emotional eating is low, Constant Hunger is moderate, and Feasting is
high
Their primary eating behaviour is Feasting, and their secondary driver
is Continuous Hunger, with some degree of overlap. Such a pattern
can help guide conversations about what is most relevant or helpful to
focus on when starting a weight-loss journey.
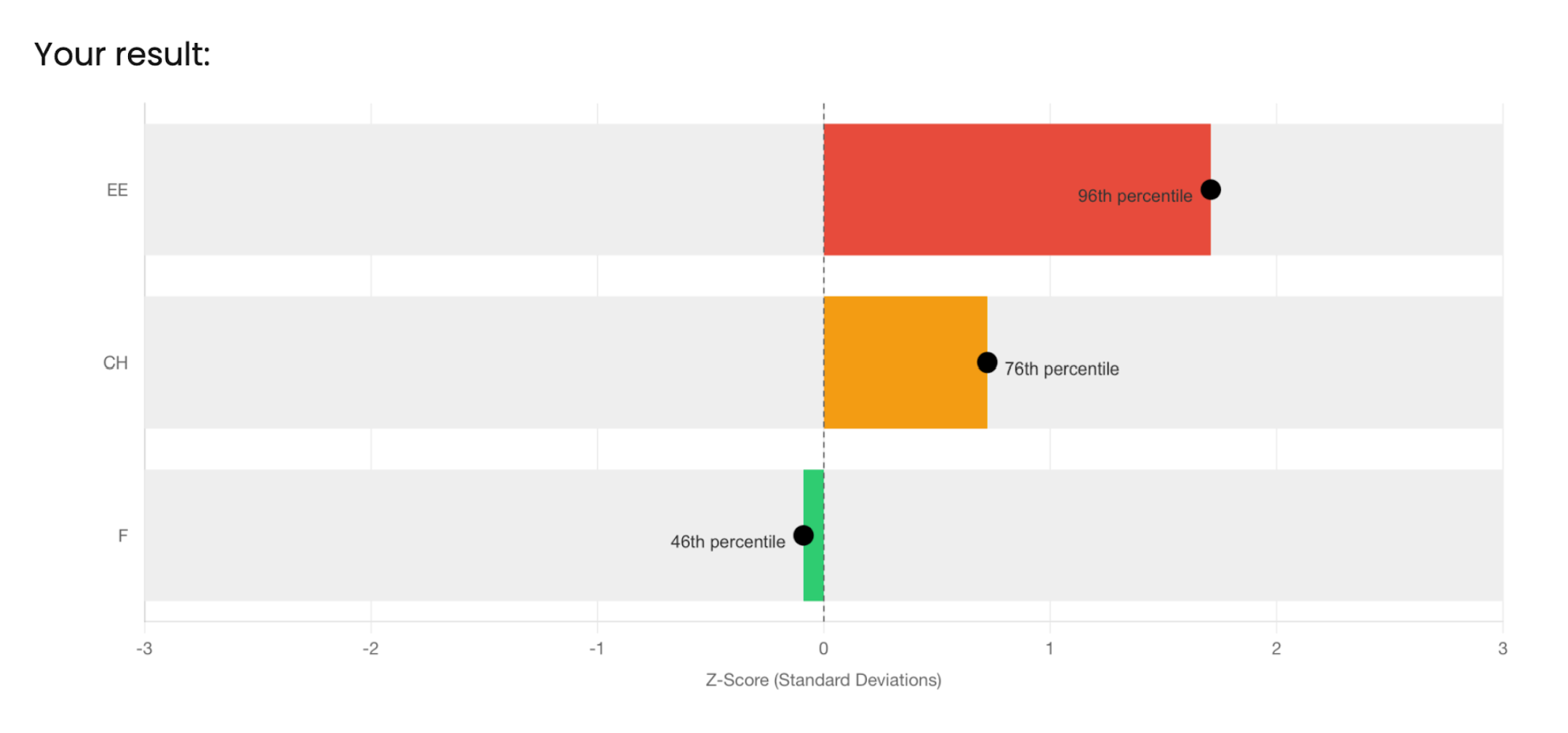
Bar Chart - Z Scores
Your results:
How to understand this chart
This chart shows how your results compare with those of other people who have taken the same test.
Each bar shows whether your score on a particular eating behaviour trait is higher or lower than most people, and by how much.
In detail
The vertical dashed line at zero shows the average score of all other people who have taken the same test
Bars extending to the right mean your score is above average.
Bars extending to the left mean your score is below average.
The length of the bar shows how far from average your score is.
For example:
Compared with the reference population, this individual shows
a very high score on Emotional Eating, a slightly-above-average
score on Constant Hunger, and a clearly below-average score
on Feasting.
This result should be interpreted in conjunction with the
individual Visual Analogue Scales (graph 1).
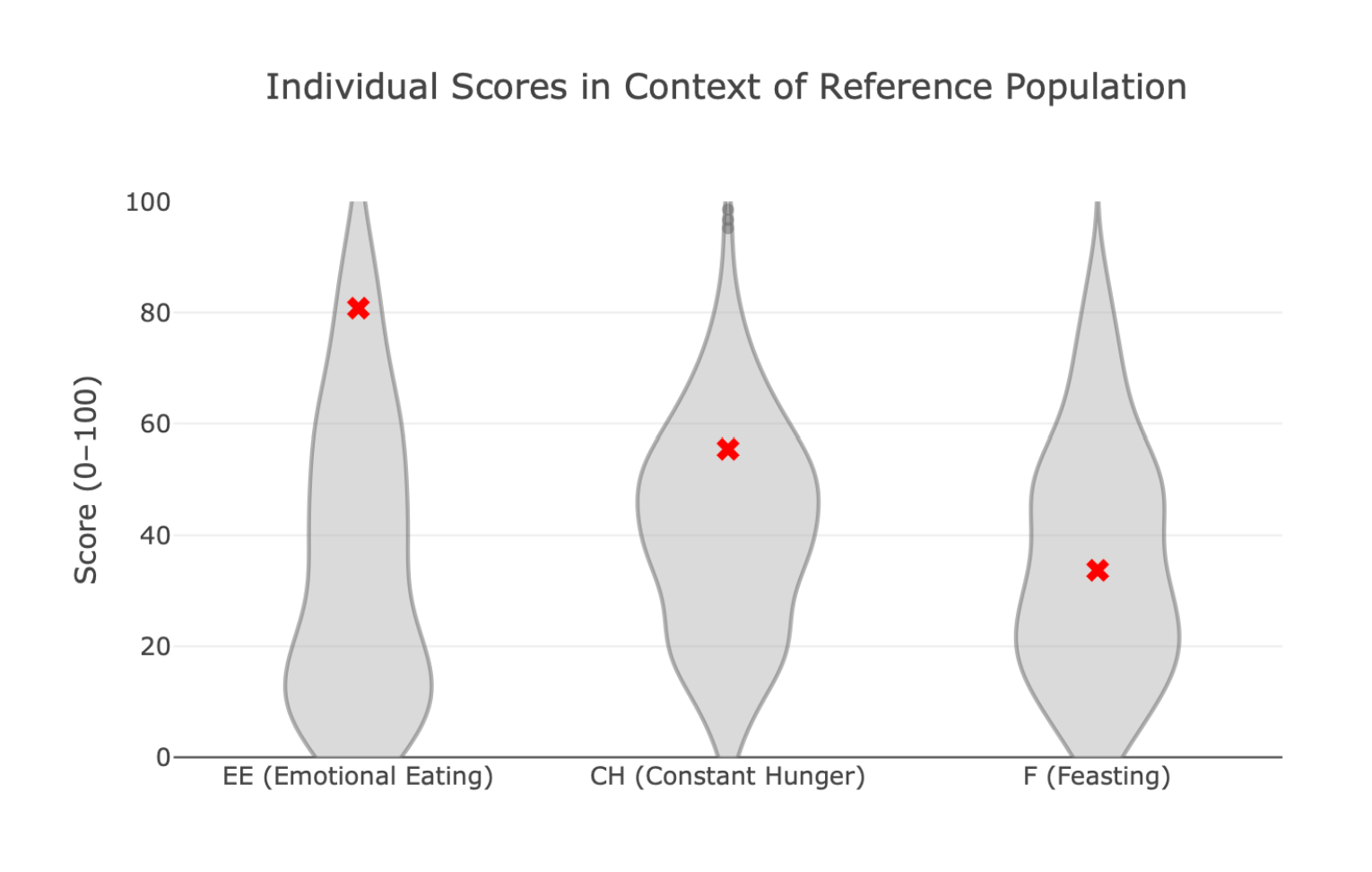
Violin Plot
Your results:
How to understand this chart
This chart shows how your results compare with those of others who
have taken the same questionnaire.
The shaded shape shows where people’s scores fall.
The wider parts of the shape mean more people scored there.
The RED dot marks your own score.
Where your dot sits within the shape shows whether your score
is lower, typical, or higher when compared with others.
For example:
For this person, the results show stronger Emotional Eating than most
others, a Constant Hunger score like that of most people who took the
test, and a lower score than most in Feasting.
The results should be interpreted together with the individual visual
analogue scales.
Scatter Plot
Your results:
General information:
Each dot on the graph represents one person. The position of the dot shows
that person’s eating behaviour score (along the bottom) and their body mass
index, or BMI (up the side).
The large RED DOT shows where your value sits in relation to all others who
have taken the test.
Overall, the distribution of points suggests a relationship between eating
behaviour score and BMI, with the BMI tending to increase as eating behaviour
scores increase.
However, people with similar eating behaviour scores can have different BMI
values.
This means that knowing someone’s eating behaviour score does not reliably
predict their BMI, and that eating behaviour is only one factor among many that
influence body weight.
Many other factors, such as genetics, metabolism, physical activity, health
conditions, and environment, also play important roles in determining a
person’s BMI.
How to interpret the results:
Option A:
If your individual value (RED DOT) is above the average line (red line in the middle of the graph),
your body mass index (BMI) is higher than average for people with a similar eating behaviour
score. In simple terms, compared with others who have a similar eating behaviour score, your
BMI is greater.
This shows that, for you, other factors, such as genetics, metabolism, medications, health
conditions, physical activity, sleep, or life circumstances, are likely contributing to a higher BMI
than would be expected based on your eating behaviour alone.
Option B:
If your individual value (RED DOT) is below the average line, your body mass index (BMI) is lower
than average for people with a similar eating behaviour score. Hence, compared with others who
have a similar eating behaviour score, your BMI is lower (you are leaner).
This result shows that your dominant eating behaviour is the driving factor for weight gain, and
working on your dominant eating behaviour with lifestyle or medication might be the best
approach for you.
About the New Zealand Eating Behaviour (NZ-EBQ) calculator
The NZ-EBQ calculator is intended to provide a guide to help you understand your unique eating behaviour type. It can show your primary and secondary drivers of eating and put them in the context of your body mass index. It also compares your results with those of hundreds of others who have already taken the test.
It can also show that your eating behaviour may be impacting your life and can be the starting point for a discussion with your healthcare provider.
Use your score to start or redirect your weight loss journey. The NZ-EBQ calculator is currently open access and free to use by anyone interested in their unique eating behaviour, whether they are on obesity medications.
It does not give or replace medical advice or medical information. Your eating behaviour score is not a diagnosis of a particular medical condition or of the underlying causes of your weight, as your weight will be affected by many other factors, such as genetics, metabolism, medications, health conditions, physical activity, sleep, or life circumstances.
There are no ‘good’ or ‘bad’ results; the questionnaire is designed to describe eating patterns, not to judge or diagnose. Your responses may help guide future discussions, support options, or research related to eating behaviour.
You should always talk to your doctor or other healthcare professional about any health problems you may be suffering from.
Eating behaviours can change over time, and these results represent a snapshot, not something that is fixed.
Tracking your eating behaviour over time can help you to understand how any intervention, whether that’s diet, medication, or lifestyle changes, impacts your eating.
It also lets you make data-driven decisions about which changes work for you.
Our research (https://pubmed.ncbi.nlm.nih.gov/41445978/) shows an association between individual eating behaviour scores and successful use of certain medications, suggesting that eating behaviour matched medication choice doubled the likelihood of success.
Repeat your calculation after making changes, to track your score over time and see what’s working.
The test was validated in over 1000 men and woman with a wide range of starting weight and different ethnicities and recently tested in people using prescribed obesity medication.
With key insights from this research, we created a new and improved version, called the NZ-EBQ calculator, which can be used by patients, clinicians, and researchers to drive forward the research about EB and how they impact weight management.
The four appetite questions at the start were designed to capture how you were feeling in the moment you completed the questionnaire.
They ask about your current level of hunger, how full you feel, and how strong your desire to eat is. Each question examines a slightly different aspect of appetite, but together they provide an overall picture of your immediate appetite state. Your answers are combined to create an overall appetite score.
This score helps us understand whether you are coming into the main part of the assessment feeling generally hungry or comfortably satisfied. This information can influence how you respond to later eating-related questions.
By measuring appetite at the start, we can take your current appetite into account when calculating and interpreting later results. This step helps ensure that any findings reflect your typical eating behaviours and responses, rather than being overly influenced by how hungry or full you happened to feel at that moment.
Eating behaviour traits are relatively stable patterns in how we experience appetite and regulate eating. A large body of evidence shows that these traits meaningfully influence body weight and weight change over time.
The NZ- EBQ measures EB traits that are related to aspects of eating that are less under voluntary our control (inert drivers of eating) such as satiety responsiveness (the awareness internal fullness signals), which is linked with overeating at mealtimes; emotional eating, which is eating in response to emotions such as stress, sadness, or boredom rather than hunger, and hunger, which consists of the intensity of feeling hungry and the time to return to hunger after a meal.
There are many other eating behaviour traits more closely related to judgement or voluntary behaviour, such as food responsiveness, enjoyment of food, planning and monitoring, restraint and its opposite, disinhibition, and external cue eating or variety seeking. Such behaviours can change and are less reliable measures for treatment selection but may be important and complementary.
We will use the answers you provide to calculate your unique eating behaviour score and to provide you with a summary of your information on how your score compares to others.
By using the NZ-EBQ calculator, you consent to us using your information for this purpose. We do not share that information with any third party other than the service providers who securely holds the data.
With your consent (optional), we will use your data for non-commercial research purposes. For example, we may publish research into eating behaviours that uses this information; however, this is not a research study. We may also use it to improve the NZ-EBQ.
You may withdraw that consent at any time by contacting …. Give e-mail.
We will not keep your information longer than the purposes for which we collected it. If you give your consent for research purposes, because our research is intended to be long-term, we are currently unable to set a specific time limit. But we will keep it under review and ensure that your information is kept no longer than necessary.
Further information about your rights in relation to your data and how to contact us are set out in our Privacy Policy.